Oral Presentation 33rd ASM of the Australian & New Zealand Bone & Mineral Society 2023
Measures of physical function are associated with increased fracture and mortality risk (#66)
Poor physical performance as measured by common tests increase the risk of fracture. However, those unable to perform these tests have the highest risk, suggesting that qualitative measures might be useful. This study investigated the association between self-assessed physical function and fracture risk.
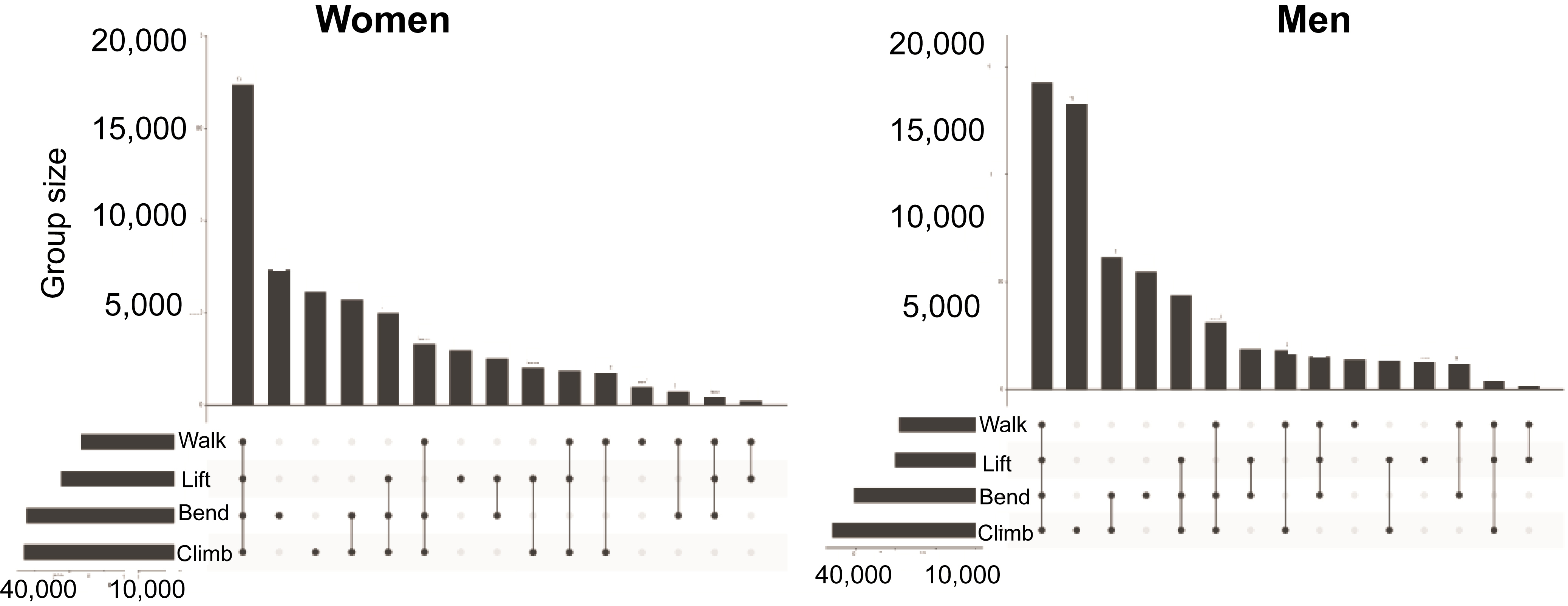
45 and Up is a population-based cohort of 116,001 people with baseline questionnaire data linked to hospital, emergency, and mortality datasets. Four self-reported measures of physical function (PF), walking, lifting, climbing stairs and bending were analysed. Fractures were identified from hospital admission and emergency presentations and mortality from vital statistics data over 5 years.
Association of PF and fracture risk was determined using cause-specific Cox models; a competing risk approach which produces simultaneous estimates of fracture and mortality. The models were adjusted for fracture risk factors and stratified by age (< 75, ≥ 75).
Approximately 20% of participants reported limitation in all PF domains (Figure). There were 7190 fractures and 4958 deaths in women and 4267 fractures and 7845 deaths in men. All PF domains were associated with increased risk of fracture and mortality. Those who reported a limitation in all 4 PFs had the highest risk. In those < 75, the hazard ratio was 1.73 (1.58 – 1.89) for fracture and 1.21 (1.12 – 1.32) for death in women and 1.64 (1.45 – 1.86) and 1.28 (1.19 – 1.37) in men. In those ≥ 75, the respective hazard ratios for fracture and death were 2.16 (1.88 – 2.47) and 1.46 (1.34 – 1.60) in women and 2.44 (2.09 – 2.84) and 1.50 (1.40 – 1.58) in men.
PF limitation is common and is associated with increased fracture and mortality risk. This study suggests that simple self-assessments may be a useful tool to select candidates for further investigation.